1Central Medical College, Comilla, Bangladesh; 2Department of Physiology, Chittagong Medical College, Chittagong, Bangladesh; 3Department of Bio Chemistry, Chittagong Medical College, Chittagong, Bangladesh; 4Department of Medicine, Chittagong Medical College, Chittagong, Bangladesh
![]() 10.3329/bmrcb.v45i2.42541
10.3329/bmrcb.v45i2.42541 ![]() 0000-0003-0300-7817
0000-0003-0300-7817
Background: Lung function varies with the different body posture of normal individuals. Normal healthy school children adopt different body posture which influences their lung function. This cross sectional observational study was done to assess the effects of different sitting postures on lung function like forced vital capacity (FVC) in healthy school children.
Methods: This study was conducted in the Department of Physiology, Chittagong Medical college, Chittagong and K S Nazu Miah High school, Khondokia, Younus Nagar, Hathazari, Chittagong during July 2015 to June 2016. A total of 88 subjects of which 42 male and 46 female students aged between 14-16 years studying in class eight to ten were included by purposive sampling method. FVC were recorded by portable digital spirometer (HI-101, Japan). Data were taken in normal upright sitting, kyphotic and at slumped sitting posture. Unpaired and paired t test and repeated measure ANOVA tests were done using SPSS for windows version 20.
Results: The mean value of FVC were significantly (p<0.001) changed in different sitting posture. Kyphotic sitting posture showed no significant difference (p˃0.05) comparing to normal upright sitting posture. Regarding slumped sitting posture comparing to normal upright showed significant low values (p<0.001). Female subjects showed significant low FVC (p<0.001) comparing to male subjects.
Conclusion: The results of this study suggest that the lung function like FVC is significantly decreased in slumped sitting posture.
Keywords: Lung function test, Forced vital capacity, Sitting posture, Kyphotic sitting posture
Lung function in children serves as a basis for health and disease.1 During childhood and adolescence there is a relation between anatomical and physiological growth of lung, chest cage and airway.2 Back pain is very common in adolescents by different sitting posture that can be prevented by introducing back care advice in primary and secondary curricula.3 Pulmonary function test is important for assessment of lung disease in children.4 Asthmatic children usually suffer from poor pulmonary function.5
Many factors can contribute to poor lung function including smoking, asthma, allergy, chronic obstructive pulmonary disease (COPD) obesity etc.6 Pulmonary function tests (PFT) are influenced by geographic, genetic, ethnic, socio-economic, life style and technical factors.7A significant relation between posture, anthopometry with lung functions has been observed in different studies.6,7
Pulmonary function was altered in school children seated leaning forward and backward.8 It was supposed that school furniture had a strong relationship with back pain & neck pain. Chair height, backrest height and position were associated with pain.9 Flexed or static posture for prolonged period may cause increased muscular fatigue in the neck and back also.9
Vital capacity showed improves in supine posture comparing to sitting posture.10Tsubak et al in their study observed that limited chest wall motion and abdominal pressure by posture change had no effect on VC and FVC in healthy young female subject.11 Functional residual capacity (FRC) was found lower in sitting position comparing to standing position.Also from sitting to recumbent and from recumbent to trendelenburg position it was gradually decreased. The changes were supposed to be due to change in expiratory reserve volume.12 The prone position showed compression of the anterior ribs causing limitation of the volume of air entry and exit to & out of the lungs.13 According to Sajal De et al obstructive airway disease showed a change in forced vital capacity (FVC) in standing posture in adult though it was insignificant.14
Still there is controversy regarding the effect of posture on lung function. In Bangladesh, school children have to sit on stool and adopt different sitting posture for prolong period. Prolonged slumped sitting posture may influence thoracic malformation. Many respiratory conditions because of structural deformities can be prevented by correcting posture at early phase of development. So, the aim of this study wasto find out any effect of different sitting posture on lung function in healthy school children. So that a new formulation about sitting furniture and device as well as advice regarding the posture can be given to school children for their better lung function and also to reduce back pain, neck pain & problem in vertebral structure.
This cross-sectional observational study was conducted in the Department of Physiology, Chittagong Medical College, Chittagong and K S Nazu Miah High school, Khondokia, Younus Nagar, Hathazari, Chittagong from July 2015 to June 2016.All subjects were selected by purposive sampling method. Boys and girls aged between 14-16 years students who were interested to participate were included in this study. Previous history of respiratory diseases, active illness, cleft lip and palates, deviated nasal septum, kyphosis, lordosis, scoliosis, respiratory depressant drug users, history of surgery were excluded. The protocol of this study was approved by Ethical Review Committee of Chittagong Medical College, Chittagong, Bangladesh.
After selection and proper counseling, the aim, objectives, lung function, different sitting posture and the procedure of the study was explained in details to all subjects. The procedure of participation in the study and detail of the lung function test were explained to them. They were encouraged for voluntary participation. The subjects were allowed to withdraw themselves from the study if they like. A written consent was taken from all the subjects included in the study and detailed personal information, medical and family history was recorded in a preformed standard case record form.
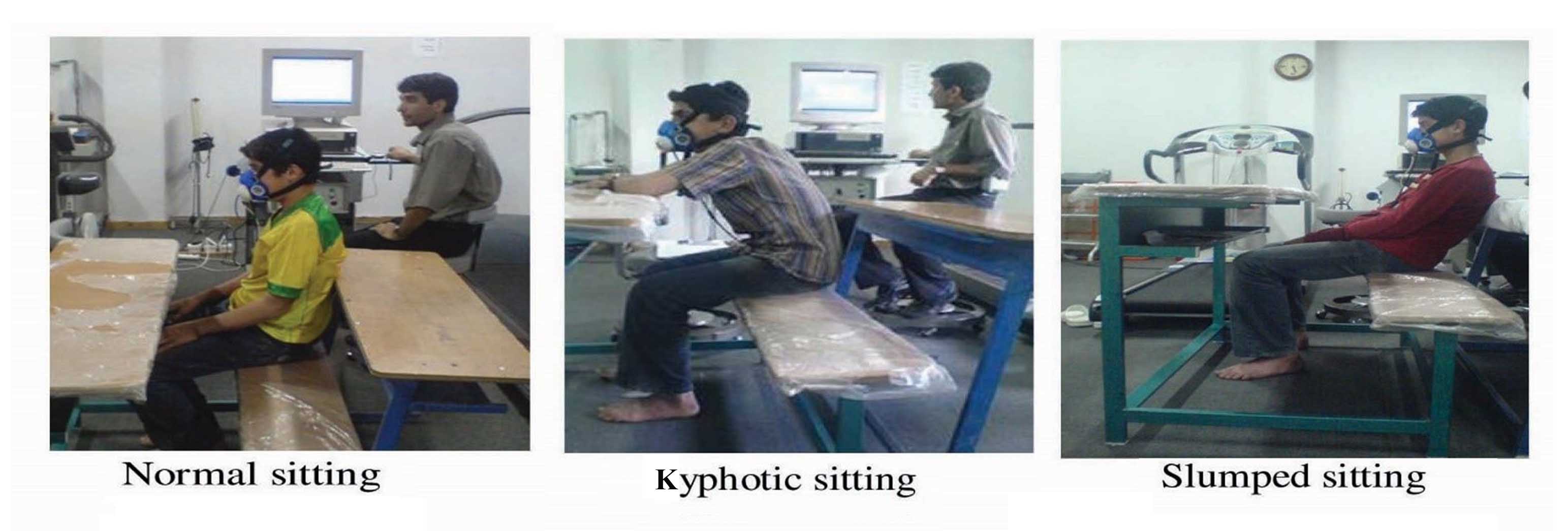
Diagram 1: Different sitting posture8
Data were collected in the class room in the presence of class teachers at break hour of school time in Saturday and Monday. Each day spirometric test was done on ten students. Height and weight were measured. Body Mass Index (BMI) was calculated by weight in kilogram divided by height in square meter.15Anaemia, jaundice, cyanosis and edema were observed. Lung function like FVC was recorded by spirometer (HI-101, Japan). Readings were taken in normal upright sitting, slumped and at kyphotic sitting postures.
The study subject was asked to take rest sitting on a stool and remain calm and quiet for 5 minutes. The detailed procedure was explained to the subject. Mouthpiece of the spirometer was cleaned with alcohol and cotton and then the mouthpiece was placed in between the lips.16 The subject was asked to hold the mouthpiece in his hand horizontally. To make good seal, the subject was asked to put the lips tightly around the outside of the mouthpiece. The switch of spirometer was on and window (dialog box) was opened. Subject was asked to inhale as deeply and rapidly as possible. Then he was asked to exhale as forcefully as possible for possible longest period into the mouthpiece. The readings of measured, predicted, and percentage of predicted values of FVC, was recorded from the spirometer monitor. Three consecutive readings for each parameter were taken and the best value was noted.
All the data were compiled and processed after collection. Then the data were analysed using SPSS-20 (SPSS Inc, Chicago, IL, USA). FVC was analysed by student t test and repeated measure ANOVA test.
The mean (± SD) age of the subjects were 15.30 (± 0.74) years. The mean (± SD) height of the subjects was 157.51 (± 7.19) cm and weight was 44.02(± 5.69) kg. The mean (± SD) BMI of the subjects were 17.84 (± 1.50) kg/m2 (figure 1).
Values expressed as mean ± SD, n = number of the subjects.
Figure 1: Age, height, weight and BMI of the study population (n=88) Values are expressed as percentage. %= Percentage
Among the total 88 subjects 42 (47.7%) were male and 46 (52.3%) were female (Figure 2). Mean (± SD) FVC of the subjects was 2.53 (± 0.13 liter in normal upright sitting posture, 2.52 (± 0.13liter) in kyphotic sitting posture and 2.40 (± 0.16) liter in slumped sitting posture. Repeated measure ‘ANOVA’ test was done to see the effects of different sitting posture on lung function. The mean FVC was significantly (p<0.001) changed in different sitting posture (table I).
Values are expressed as percentage. %= Percentage
Figure 2: Sex distribution among the study population.
Among the total 88 subjects 42 (47.7%) were male and 46 (52.3%) were female (figure 2). Mean (± SD) FVC of the subjects was 2.53 (± 0.13 liter in normal upright sitting posture, 2.52 (± 0.13liter) in kyphotic sitting posture and 2.40 (± 0.16) liter in slumped sitting posture. Repeated measure ‘ANOVA’ test was done to see the effects of different sitting posture on lung function.The mean FVC was significantly (p<0.001) changed in different sitting posture (table I).
Postures |
FVC(L) (Mean± SD) |
p value |
|---|---|---|
Normal upright sitting |
2.53 ± 0.13 |
<0.001*** |
Kyphotic sitting |
2.52 ± 0.13 |
|
Slumped sitting |
2.40 ± 0.16 |
Results are expressed as mean ± SD. p value was obtained by repeated measure ANOVA test. n = number of the subjects. L indicates litre. * marks signify significance of tests.
The Paired student’s ‘t’ test was done to compare between different sitting posture. Mean FVC in kyphotic sitting posture comparing to normal upright sitting posture was not statistically significantly. Significant low FVC (p<0.001) was observed in slumped sitting posture comparing to normal upright sittng posture (table II).
Postures |
FVC(L) (Mean±SD) |
p value |
|---|---|---|
Normal upright sitting |
2.53 ± 0.13 |
0.06 |
Kyphotic sitting |
2.52 ± 0.13 |
|
Normal upright sitting |
2.53 ± 0.13 |
<0.001 |
Slumped sitting |
2.40 ± 0.16 |
Results are expressed as mean ± SD, n = number of the subjects. * marks signify the test of significance. p values were obtained by Paired student’s ‘t’ test was done.
Unpaired student’s ‘t’ test was done between male and female. In female subjects significant low FVC was observed comparing to male subjects in different sitting posture (p<0.001) (table III).
Postures |
Male (n=42) |
Female (n=46) |
p value |
|---|---|---|---|
Normal upright sitting |
2.61 ± 0.12 |
2.45 ± 0.10 |
<0.001 |
Kyphotic sitting |
2.60 ± 0.11 |
2.44 ± 0.09 |
<0.001 |
Slumped sitting |
2.48 ± 0.15 |
2.34 ± 0.13 |
<0.001 |
Results are expressed as mean ± SD. n = number of the subjects. * marks signify significance of tests. p values were obtained by Unpaired students ‘t’ test.
The present study was done to assess the lung functions among the healthy school children in different sitting postures. Anthropometric measurement of the subjects such as height, weight and BMI were measured. FVC were taken by using digital spirometer in upright, kyphotic and slumped sitting posture to see the lung function. Repeated measure ANOVA and paired ‘t’ test were done as test of significance.
In this study, significant changes of FVC in different sitting posture of the study sample were observed (p<0.001). These values were significantly decreased in slumped sitting posture than normal and kyphotic sitting posture. These results were consistent with the findings of Hozat and Mahdi and Lin et al In their studies slumped sitting posture showed a decreased values of pulmonary function than other posture.6,8 This might be due to increase intra abdominal pressure affecting lung expansion and limitation of dorsal chest wall in slumped sitting posture.8 Size of free airway also is affected by the head flexion and extension. Position of the head and neck in proper alignment reduces airway obstruction which helps in increase pulmonary function.In slumped sitting posture another possible reason for the lowest FVC may be the position of the head posture.8 Lin et at found lowest lumber lordosis recorded in the slumped sitting posture.6 They reported that significant difference inlumber lordosis in different sitting posture may account for changes in the pulmonary capacity between the posture.6 Probably our findings may also due to this cause.
Findingsof the study,dissimilar with the findings of some investigators. They found no effect on pulmonary function in upright andslumped sitting posture in young healthy individual in their study.Though they found upright sitting posture had better pulmonary function than other sitting posture but it was not significant.17
According to Chowdhury PR et alvital capacity showed improvement in supine posture comparing to sitting posture.10 They explained that the height of the diaphragm within the thorax also varies considerably with posture. Diaphragm remains at highest position when the body is in supine position and performs the largest respiratory excursions with normal breathing.10 In sitting posture, the diaphragm remains at lowerposition and the respiratory excursions become smaller. Also in supine posture the scope of diaphragmatic movements increases. As a result, vital capacity showed greater value in supine posture in their study.10
In this study, it was tried to compare FVC in boys and girls. It was observedsignificant low values of FVC in female children comparing to male. This findings is consistent with some previous findings.17-19 They showed sameheight matched boys had greater lung function values comparing to girls.1It might be due to that female children had reduced lung volumes and capacities due to their body configuration such as decreased lung size and airways comparing to male children.11,19 It was supposed that reduced lung size, reduced muscle power, decreased maximal respiratory flow rates, reduced airway diameter and smaller diffusion surface was the cause of low values.11,19,20
Conclusion
By this study it can be concluded that different sitting posture has effect on lung functions like FVC and male children have higher values of FVC compared to female children.
References
- Nagpal S, Thaman RG, Bachhel R, Monga U. Study of Forced Vital capacity in healthy school children of Amritsar District, Punjab. Sch J App Med Sci 2013; 1(4):252-55.
- Chowgule RV, Shetye VM, Parmar JR. Lung function test in normal Indian children. Indian pediatr 1995; 32(2):185-91.
- Prendeville K, Dockrell S. A pilot survey to investigate the incidence of low back pain in school children. Physiotherapy Ireland 1998; 19(1):3-7.
- Couriel JM, Child F. Applied physiology:lung function testing in children. Current paediatrics 2004; 14:444-51
- Begum JR, Islam MI, Matin A. Spirometric lung function test in school children with asthma. J Bangladesh Soc Physiol 2010 Dec; 5(2):75-79.
- Lin F, Parthasarathy S, Taylor S, Pucci D, Hendrix R, Makhsous M. Effect of different sitting postures on lung capacity, expiratory flow, and lumbar lordosis. Arch Phys Med Rehabil 2006; 87(4):504-509.
- Budhiraja S, Sing D, Pooni PA, Dhooria GS. Pulmonary functions in normal school children in the age group of 6-15 years in North India. Iran j Pediatr 2010; 20(1):82-90.
- Hojat B, Mahdi E. Effects of different sitting posture on pulmonary function in students. Journal of Physiology and Pathophysiology 2011; 2(2):29-33.
- Murphy S, Buckle P, Stubbs D. Back pain amongst school children and associated risk factors. International Ergonomic Association XVth terminal congress. Aug 24 -29. Seoul, Korea. 2003.
- Roychowdhury P, Pramanik T, Prajapati R, Pandit R, Singh S. In health- vital capacity is maximum in supine position. Nepal Med Col J 2011; 13(2):131-32.
- Tsubaki A, Deguchi S, Yoneda Y. Influence of posture on respiratory function and respiratory muscle strength in normal subjects. J Phys Ther Sci 2009; 21:71-74.
- Blair E, Hickam JB. The effects of change in body position of lung volume and intrapulmonary gas mixing in normal subjects. The Journal of Clinical Investigation 1954; 3:383-89.
- Vilke G, Chan T, Neuman T, Clausen J. Spirometry in normal subjects in sitting, prone, and supine positions. Respir. Care, 2000; 45(4):407-10.
- Sajal De. Comparison of spirometric values in sitting versus standing position among patients with obstructive lung function. Indian Journal of Allergy, Asthma and Immunology. 2012; 26(2):86-88.
- World Health Organization. Training course on Child growth assessment WHO child growth standards, 2008.1-47.
- Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A et al.Standardisation of spirometry.Eur Respir J 2005; 26:319-38.
- Vanwala JJ, Shah S, Vyas N. Effect of different sitting postures on pulmonary function in young healthy individuals. World journal of pharmaceutical research.2015; 4(9):1396-1409.
- Ojo OA, Adeniran SA, Fatiregun O, Sunday O, Bamiwuye S. Relationship between body circumferences and lung function tests among undergraduate students of a Nigerian University. Pak J Physiol 2013; 9(1):3-6.
- Laksmi A and Kokati AB. Effect of posture on vital capacity in both males and females phase 1 medical students. Indian Journal of Basic and Applied Medical Reasearch 2015; 4(4):167-69.
- Bhatti U, Rani k, Memon MQ. Variation in lung volumes and capacities among young males in relation to height. J Ayub Med Coll 2014; 26(2):200-02.