![]() 10.3329/bmrcb.v45i1.41804
10.3329/bmrcb.v45i1.41804 ![]() 0000-0003-3162-8805
0000-0003-3162-8805
Background: Light-cured bonding systems have been widely accepted among orthodontists. Various light curing units are available now. Recently, the light emitting diode (LED) has been introduced alongside halogen light curing units. There is lack of information on the advantages and disadvantages of different light curing systems.
Objective: Objective of this in vitro study was to compare the shear bond strength of orthodontic brackets and adhesive remnant index (ARI) of an adhesive cured with two different orthodontic light sources i.e. LED and halogen.
Methods: Forty four (22 in each group) extracted human premolars without any defects were etched with 37% phosphoric acid and cleansed with water spray and air dried. The sealant (Ortho Solo) was applied on the tooth surface and the brackets were bonded using adhesive (Enlight). Adhesives were cured with Halogen (Litex) and LED (D-LUX) for 40 seconds. Then the specimens were debonded later using a universal testing machine, with crosshead speed of 0.2 mm/min until the brackets were detached. Adhesive remnant index (ARI) scores were assessed under stereomicroscope at ×10 magnification.
Results: The shear bond strength in Halogen group was 19.73 ± 3.44 MPa and in the LED group 20.81±3.02 MPa which is little higher than halogen group. The proportion of being adhesive remaining index for ARI Score 1 in Halogen group was 5 (22.7%) and in LED group 7 (31.8%). While ARI Score 2 in the Halogen group was 13 (59.1%) compared to LED group 8 (36.4%). However, ARI Score 3 in Halogen group was 4 (18.2%) and in LED group 7 (31.8%). The overall model showing no significant difference.
Conclusion: With limitations, this in vitro study showed the shear bond strength of orthodontic adhesives cured with a LED was statistically equivalent to those cured with a halogen light curing unit. There were significant differences in the ARI scores of the light-curing units tested. LED light-curing units can be suggested for the polymerization of orthodontic bonding adhesives because it showed a balanced effect on ARI index.
Keywords: Shear bond strength, Light curing unit, LED, Racket bondingOne of the most significant advances in orthodontics in the past 3 decades is the use of composite resin as a bonding material.1 Bonding with light activated systems is popular because the extended working time, which allows for precise bracket placement.2,3
Blue light generated by conventional halogen light curing units has typically constituted the most popular method of bonding orthodontic adhesives for many years.4
Halogen bulbs produce light when electric energy heats a small tungsten filament to high temperature.5 However, tungsten-quartz halogen curing units have several shortcomings. These shortcomings include the narrow range of light, limited to visible wave lengths and represents only a small part of the entire electromagnetic spectrum ranging a wave length from 455 nm to 492 nm. Only 1% of the total energy emitted is converted to light with the remainder generated as heat.4,6 The short life of halogen bulbs and the noisy cooling fan are other disadvantages. Moreover, it requires more time than LED light for complete polymerization for resin.
So, Mills and Nakamura et al proposed the LED (light-emitting-diode) as an alternative to the halogen curing light.4,7 This device, instead of using a heated tungsten filament, has two solid semiconductors joined together, and an electric charge is applied using a battery.7 When electrons and holes meet, energy is released in the form of light and therefore generates minimal heat and the fact that they have 10,000 hours lifetime with little degradation of output.8
Several studies were unable to demonstrate a significant difference between the adhesion forces obtained with an LED light-curing device as compared to that achieved using a halogen light. However, other studies have reported a lower bond strength when the LED lamp was used for the limited period of 10 seconds. Clinically acceptable adhesion force is over 8 MPa.9 In 1975, Reynold suggested that at least 6-8 MPa bond strength is acceptable clinically.10 Ross S Hobson et al showed that the shear bond strength was significantly differ between the dry etched enamel and the etched surface were contaminated with water or human blood.11 But as this was an in vitro study, no scope of etched surface contamination was possible. Previous studies have shown that LED-curing units are as effective as halogen-based sources.5 In 2006 Abtahi SM et al found no significant difference in bond strength between the LED and halogen groups (p=0.12).12 However, the mean shear bond strength of the LED group (19.74 MPa) was higher than the halogen group (16.6 MPa). Where as in 2010 Di Nicoló Ret al. also found no significant difference in bond strength, but bond strength of halogen group (20.01±5.24 MPa) was higher than LED Group (17.35±5.07 MPa).13
Atmadja and Bryant carried out a study evaluating the micro-hardness of four resins (P30, Prisma-Fil, Heliomolar and Durafil).14 They concluded that: a) the micro-hardness values decreased with the increasing depth of polymerization, b) the most effective exposure time was 40 seconds, c) reducing the thickness is better than to increase the exposure time d) polymerization reaction continues even after the light source is removed.
Although there are few studies in the literature, it is believed that the LED device has real conditions of replacing halogen devices in offices. The light-curing devices with halogen lamps have a vast literature on the subject, unlike LEDs, which are currently being investigated more intensely. As far as we know no previous research regarding this topic was performed in this country. With this in mind, the study will be an endeavor to compare the effect of LED and Halogen light curing systems on the shear bond strength of orthodontic brackets.
The test sample consists of 44 (forty four) human mandibular and maxillary premolars. Teeth with any irregularities of the enamel surface had excluded from the study and were stored in saline solution.
Each tooth was mounted vertically in acrylic resin block with the long axis of each tooth set vertically and the crown remaining exposed (figure 1).
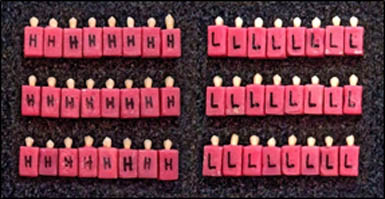
Figure 1: Sample teeth mounted vertically in auto polymerizing acrylic resin block
Then buccal surfaces of the teeth were cleaned with pumice and then washed with water. Before bonding, the sample was randomly divided into two groups.
Then these teeth were etched with 37% phosphoric acid and cleansed with water and air dried. Then a thin layer of orthodontic adhesive primer (Ortho Solo) had applied on the tooth surface and metal brackets (Stainless steel Roth, Ormco) had bonded using adhesive (Enlight), and all excess resin on the edges of the bracket was thoroughly cleaned before polymerization. Then- Group I adhesives were cured with halogen light (Litex, Dentamerica) and Group II adhesives were cured with the LED light (D-Lux, Diadent, Korea) for 40 seconds (20 seconds from the mesial and 20 seconds from the distal sides) and stored in distilled water for 24 hours.
Then the shear bond strength of the specimens was evaluated with a Universal testing machine (Tinius Olsen, Hounsfield-H10KS, 500N sensor) (figure 2).
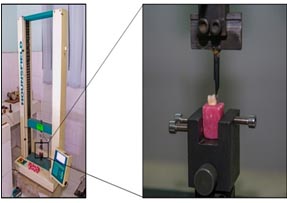
Figure 2: Universal testing machine (Hounsfield-H10Ks, USA) holding the sample, secured in a jig attached to base plate.
Before debonding, the embedded specimens were secured in a jig attached to the base plate of universal testing machine. A chisel-edge plunger was mounted in the movable crosshead of the testing machine and positioned such that the leading edge aimed the enamel-adhesive interface before being brought into contact at a crosshead speed of 2 mm/min. An occlusogingival load was applied to the bracket producing a shear force at the bracket-tooth interface. A computer connected with the machine recorded the results of each test. The force required to dislodge the brackets was measured in Newton (N), and the shear bond strength (SBS) was calculated in Megapascal (MPa) by dividing the force values by the bracket (Roth 0.022, Ormco) base areas (3mm × 3.5mm = 10.5mm2).
After debonding adhesive remaining index (ARI) scores were examined with a stereomicroscope (magnification×10) by one investigator based on scores given by Artun and Bergland in 1984 (figure 3).
Score 0 = No adhesive left on the tooth.
Score 1 = Less than half of the adhesive left on the tooth.
Score 2 = More than half of the adhesive left on the tooth.
Score 3 = All adhesive left on the tooth, with distinct impression of the bracket mesh.

Figure 3: Adhesive remaining index (ARI) Scores viewed under Stereomicroscope.
Independent sample t-test was performed to see the shear bond strength between light curing methods Halogen and LED. Chi-square test was performed to compare the adhesive remaining index (ARI) scores of the bonding material after debonding between the two groups. ANOVA model was used to see the relation of ARI with shear bond strength in overall group and within the Halogen and LED groups. p- Value was considered at p≤0.05.
The study was performed with 44 (22 in each group) non-carious human premolars (both maxillary and mandibular) extracted for orthodontic purposes in the department of orthodontics, BSMMU in the year 2016. Adhesives were cured with the halogen and LED light for 40 seconds (20 seconds from the mesial and 20 seconds from the distal sides) and stored in distilled water for 24 hours (table I).
Group |
Light-curing systems |
Curing times |
Number of sample |
|---|---|---|---|
1 |
Halogen |
20 seconds mesial, 20 seconds distal |
22 |
2 |
LED |
20 seconds mesial, 20 seconds distal |
22 |
Independent sample t-test was used to see the Shear bond strength between the two groups. The Shear bond strength in Halogen group was 19.73±3.44 MPa and in the LED group it was 20.81±3.02 MPa. No significant difference was noted between the shear bond strength acquired with Halogen and LED (table II and figure 4).
Light-curing systems |
Mean ± SD |
95% confidence Intervals (CI) |
p-value |
|
|---|---|---|---|---|
Lower bound |
Upper bound |
|||
Halogen (n=22) |
19.73±3.44 |
18.34 |
21.12 |
0.274 |
LED (n=22) |
20.81±3.02 |
19.42 |
22.20 |
|
The proportion of being adhesive remaining index for ARI Score 1 (less than half adhesive remain in the teeth) in Halogen group 5 (22.7%) and in LED group 7 (31.8%) (Table III). While ARI Score 2 (more than half of the adhesive left on the tooth) in the Halogen group was 13 (59.1%) compared to LED group 8 (36.4%). However, ARI Score 3 (all adhesive left on the tooth, with distinct impression of the bracket mesh) in Halogen group 4 (18.2%) and in LED group 7 (31.8%). The overall model showing no significant difference p=0.310 (table III and figure 5).
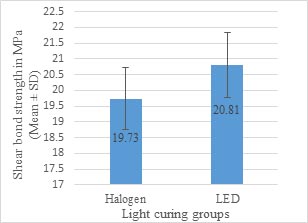
Figure 4: Bar diagram showing comparison of (Mean ± SD) the Shear Bond Strengths between the Halogen and LED group
Data is presented as mean ± standard deviation and 95% confidence interval (CI). p<0.05 was consider as significant.
Adhesive Remaining Index (ARI) |
ARI Score |
Light-Curing groups |
Total (n=44) |
χ2 |
p-value |
|
|---|---|---|---|---|---|---|
Halogen, |
LED, |
|||||
Less than half of the adhesive left on the tooth, n(%) |
1 |
5 (22.7%) |
7 (31.8%) |
12 (27.3%) |
2.32 |
0.310 |
More than half of the adhesive left on the tooth, n(%) |
2 |
13 (59.1%) |
8 (36.4%) |
21 (47.7%) |
||
All adhesive left on the tooth, with distinct impression of the bracket mesh, n(%) |
3 |
4 (18.2%) |
7 (31.8%) |
11 (25.0%) |
||
Data is presented as number with percentage in parentheses.
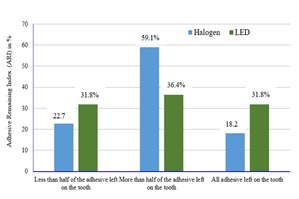
Figure 5: Distribution of Adhesive Remaining Index (ARI) in the two Light-Curing groups. No adhesive left on the tooth in the both group was not detected.
There is a significant difference between the highest and lowest ARI score with SBS in overall group (p=0.005) and LED group (p=0.02) respectively (figure 6). While for halogen group there was no significant association (p=0.06) noted between the score 1 and score 3.
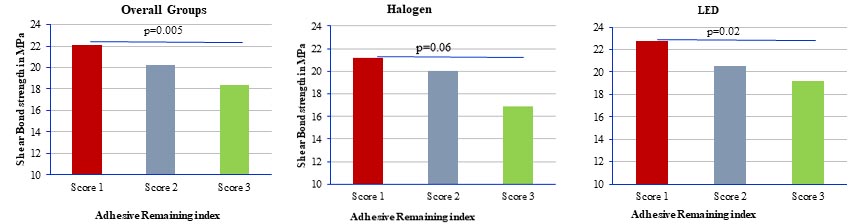
Figure 6: Association between ARI and SBS in overall and Halogen and Led group.
The in vitro use of light-cured materials for direct orthodontic bonding was first described in1979.15 In the direct bonding technique, the material is cured under metal-based brackets by direct illumination from different sides and by transillumination, because the tooth structure transmits visible light. A rapid polymerization occurs when visible light is applied, such setting “on demand” results in a nearly unlimited working time, allowing more accurate bracket placement.8
The study was designed to comparative evaluation of the shear bond strength values of orthodontic brackets bonding to teeth after being cured with LED and halogen lights and also differences in adhesive remaining index (ARI) scores of the bonding material after debonding.
The present study showed no statistically significant differences between the groups, thus demonstrating that the type of light-curing device (halogen or LED) had no influence on the shear bond strength of orthodontic brackets. Though the light-curing device LED had little more shear bond strength compared to halogen. Previous research has shown that LED-curing units are as effective as halogen-based curing units.5,8,16 It has been previously showed that during in vitro study minimum bond strength of 16 to 20 MPa should be adequate for most clinical orthodontic needs.17 According to this minimum requirement, these two light sources cured the adhesive to an equally satisfactory level.
LEDs are being aggressively marketed; however, independent research has not yet verified the potential of this technology to replace halogen visible light–curing units.5 In 1996 and 1998 Fujibayashi et al. detected no differences in composite hardness and depth of cure between the LED and a halogen unit and obtained a deeper cure with the LED.18,19 A busy orthodontic practitioner may find them a worthwhile investment for the time being, but those have a long term benefits. The LED curing light does not have a bulb so there is no requirement for periodic replacement and there is also no potential loss of intensity in light output with time as well as reduced running costs and improved reliability.
The result of adhesive remnant Index (ARI) raveled that there is no significant difference for the both groups. The ARI scores in the present study indicate that, regardless of the type of light-curing system, most of the (score I and II) adhesive remained on the tooth after bracket debonding suggesting that the weakest adhesion occurs between the metallic bracket and the bonding material. In this vitro study we observed that a lower shear bond strength when ARI score is higher and highest shear bond strength when ARI score is lowest in overall and LED group. Bryant et al. found that the composite-bracket base interface was the weak link in the direct bonding of orthodontic attachments.20 The ARI is influenced by many factors including bracket design and tooth curvature.21
Conclusion
Based on the methodology applied in this study, and according to the results obtained and applied to the statistical analysis, it was considered reasonable to conclude that the LED light curing unit provided the highest mean shear bond strength of brackets, but without statistical significance in relation to performed with Halogen devices. Although the LED light units are cordless, smaller, and lighter with estimated lifetimes of over 10,000 hours, and they do not require a noisy cooling fan. Therefore, it seems that they are a better choice as compared to halogen light units.
Acknowledgement
The authors are thankful to the Department of Orthodontics, BSMMU for their support to conduct the study. They are also thankful to Pilot plant & PDC of Bangladesh Council of Scientific and Industrial Research (BCSIR) for their cooperation and support which made this study possible.
References
- Newman GV. Epoxy adhesives for orthodontic attachments:progress report. Am J Orthod. 1965; 51:901-3.
- Sonis AL. Comparison of a light-cured adhesive with an autopolymerizing bonding system. J Clin Orthod. 1988; 22:730-2
- McLaughlin R, Bennett J, Trevisi H (1999). Practical Techniques for Achieving Improved Accuracy in Bracket Positioning. Orthodontic Perspectives. VI-1:21-24.
- Dunn WJ, Taloumis LJ. Polymerization of orthodontic resin cement with light-emitting diode curing units. Am J Orthod Dentofacial Orthop. 2002; 122:236-41.
- Mills RW, Jandt KD, Ashworth SH. Dental composite depth of cure with halogen and blue light emitting diode technology. British Dental Journal. 1999; 186:388–91.
- Jandt KD, Mills RW, Blackwell GB, Ashworth SH. Depth of cure and compressive strength of dental composites cured with blue light emitting diodes. Dental Materials. 2000; 16:41-47.
- Nakamura S, Mukai T, Senoh M. Candela-class high brightness InGaN/AlGaN double heterostructure blue-light-emitting diodes. Appl Phys Letters. 1994; 64:1687-89.
- Usumez S, Buyukyilmaz T, Karaman AI. Effect of light-emitting diode on bond strength of orthodontic brackets. Angle Orthod. 2004; 74:259-63.
- Swanson T, Dunn WJ, Childers DE, Taloumis LJ. Shear bond strength of orthodontic brackets bonded with light emitting diode curing units at various polymerization times. Am J Orthod Dentofacial Orthop. 2004; 125:337-41.
- Reynolds IR. A review of direct orthodontic bonding. Br Dent J. 1975; 138:171-8.
- Ross SH, Jan L, John GM. The effect of moisture and blood contamination on bond strength of a new orthodontic bonding material. Am J Orthod Dentofacial Orthop. 2001; 120:54-57.
- Abtahi S M, Khamverdy Z. A Comparison of the Shear Bond Strength of Orthodontic Brackets Bonded With Light-Emitting Diode and Halogen Light-Curing Units. Journal of Dentistry, Tehran University of Medical Sciences. 2006; 3:107-111.
- Di Nicoló R, Araujo MAM, Alves LAC, Souza ROA, Rocha DM. Shear bond strength of orthodontic brackets bonded using halogen light and light-emitting diode at different debond times. Braz Oral Res. 2010; 64;24:64-69
- Atmadja G, Bryant RW. Some factors influencing the depth of cure of visible light-activated composite resin. Aust Dent J. 1990; 35:213–218.
- Tavas MA, Watts DC. Bonding of orthodontic brackets by transillumination of a light activated composite: an in vitro study. Br J Orthod. 1979; 6:207–208.
- Bishara SE, Ajlouni R, Oonsombat C. Evaluation of a new curing light on the shear bond strength of orthodontic brackets. Angle Orthod. 2003; 73:431-35.
- Turkkahramana H, Cenker H. Orthodontic Bracket Shear Bond Strengths Produced by Two High-power Light-emitting Diode Modes and Halogen Light. Angle Orthodontist. 2005; 75:854-57.
- Fujibayashi K, Ishimaru K, Kohno A. A study on light activation units using blue light emitting diodes. J Jap Dent Pres Acad. 1996; 39:180–88.
- Fujibayashi K, Ishimaru K, Takahashi N, Kohno A. Newly developed curing unit using blue light emitting diodes. Dent Jpn. 1998; 34:49–53.
- Bryant S, Retief DH, Russell CM, Denys FR. Tensile bond strengths of orthodontic bonding resins and attachments to etched enamel. Am J Orthod Dentofacial Orthop. 1987; 92:225-231.
- O’Brien K D, Watts D C, Read M J F. Residual debris and bond strength: is there a relationship? American Journal of Orthodontics and Dentofacial Orthopedics. 1988; 94: 222–230.