2Directorate General of Medical Services, Bangladesh Armed Forces, Dhaka, Bangladesh
3Combined Military Hospital, Dhaka, Bangladesh
Sensitivity pattern of isolates from patients’ specimens associated with infection, admitted to the critical care centers with empiric or prophylactic antibiotic use were assessed. Till identification of the organism and resultant sensitivity awaited; and compared with sensitive antibiotic to the isolates which could be used for management. This analytical cross sectional study carried out during the period of April 2016 to July 2016 in the Critical Care Centre (CCC) of Combined Military Hospital, Dhaka Cantonment. Urine and other specimens including wound swab, pus, sputum, tracheal aspirate, catheter tip, nasal swab, high vaginal swab, broncheoalveolar lavage, blood, urethral discharge were collected from the patients following aseptic precautions. Isolate identification was done using standard procedures at the Armed Forces Institute of Pathology (AFIP). Sensitivity was tested using antibiotic disc diffusion technique. A total of one thousand six hundred and seventy patients were dealt with in the study, and positive yield obtained in 190 (11.38%) cases. Of those, 116 were urine specimens which constituted 69 (57.76%) female and 47(42.24%) male patients. A total of 1088 discs of antibiotics were used on an average 9 discs per isolate. Six hundred and forty nine (59.65%) showed resistance to the antibiotic used against them, while four hundred and thirty nine (40.35%) showed sensitive response. The study population was of 2-80 years age group. Other specimens included 74 isolates, fifty (67.57%) were males and twenty four (32.43%) were females. A total of eight hundred and twenty seven (11.18 discs per isolate) antibiotic doses were used 479 (57.92%), showed resistant and 348 (42.08%) sensitive result. Enteric gram negative bacilli (GNB) were the majority of isolates in both types of specimens. The study indicated that, newer antimicrobials have a substantial impact in decreasing human morbidity and mortality rates. It encourages to expand surveillance of antibiotic resistance determinants and to exercise caution in dispensing antibiotics to maximize their continued efficacy. Excess or injudicious use is causing increase in cost as well as inducing drug resistance among the common bacterial isolates. A work on the clinical presentation with trends of antimicrobials used in the CCC setup right now in tertiary care hospital would be of supplemental value for the study.
Keywords: Isolate, Antibiotic resistance, Urine, Stewardship
Familiarity with evolving patterns of antimicrobial resistance in enteric gram-negative bacilli (GNB) is necessary in the selection of appropriate empiric therapy, particularly given the lag between published and real time resistance rates and the ever increasing prevalence of multidrug resistant (MDR) GNB. If broad spectrum treatment has been initiated and information on microbial susceptibility is become available, it is just as important to use the most appropriate narrow spectrum agent. This type of antimicrobial stewardship will avoid unnecessary selection of and potential super-infection with resistant bacteria, may decrease costs, and maximize the useful longevity of available antimicrobial agent.1 Likewise, it is important, not to treat patients who are colonized but not infected.2 The antimicrobial resistance profiles of GNB vary with species, geographic location, regional antibiotic use, and hospital site e.g. intensive care units (ICUs) versus wards. Rodriguez B et al showed that a comprehensive “bundle” approach for control of hospital wise endemic MDR Acinetobacter baumannii, a GNB, that could effectively control the spread and impact of MDRAb.3 Problems associated with excessive use of antibiotics were recognized shortly after their introduction into clinical use in 1940s.4 In his review on the subject in 1956, Jawetz was the first to recognize the problem caused by the attractiveness of new antibiotics to physicians, exaggerated claims by the pharmaceutical industry, and the enormous impact that promotion by the drug companies had on medical practice.5 Approximately, 60% of all hospitalized patients in the USA, receive at least one dose of an antimicrobial drug during hospitalization.6,7 It appears that as much as 50% of this use is unnecessary or otherwise inappropriate.8,9 Among the unwanted consequences of antimicrobial therapy are, increased length of hospital stay, increased cost, predisposition to secondary infections, and, most importantly the emergence of drug resistant organisms.10 Antimicrobial drug use is responsible for the rising incidence of serious health care-associated infection due to methicillin and glycopeptide resistant Staphylococcus aureus, vancomycin resistant Enterococci (VRE), extended-spectrum β-lactamase-producing Enterobacteriaceae, multidrug resistant Pseudomonas aeruginosa and Acinetobacter spp, Klebsiella spp expressing Klebsiella pneumonia carbapenemases, as well as proliferation of more virulent strains of Clostridium difficile.11-13 The increase in rates of resistance is not matched by development of antimicrobial drugs, leading to the inevitable conclusion that we must be smarter in using the drugs we currently have, to preserve their usefulness.14 The antimicrobials are “special” because their use in one patient has the potential for adverse consequences in other who has not received the drug; the usefulness of these agents is declining with their increased use; this gave rise to the term “stewardship” in 1996 to draw attention to these unique characreristics.15 Previously referred to as antimicrobial “management or “control” programmes16,17. The focus of these programs tended to be financial, because antibiotic expenditures accounted for as much as 30-50% of a hospitals total drug budget.18 Support of antimicrobial stewardship programmes (ASPs) in hospital received a major boast in 2007 with the publication of stewardship guidelines from the Infectious Diseases Society of America (IDSA).19
Antimicrobial stewardship: The programmes for improvement in the quality of patient care, with the goals of improving clinical outcomes and stabilizing or reducing rate of resistance is called Antimicrobial Stewardship Programme (ASP).20 Firstly, one must understand constrains under which physicians work and the pressure that are exerted on them to prescribe drugs. It has become more of a psychological or philosophical endeavor than a scientific exercise.21
Factors identified leading to inappropriate use of antimicrobial agents: 22,23
- ) Good intentions;
- ) Inappropriate dosing;
- ) Inappropriate prophylaxis-Hospitalized patients receives antimicrobial agents for a variety of other prophylactic purposes that are not evidence–based and that may contribute to the resistance emergence;
- ) Use of multiple antimicrobial agents or broad spectrum combinations to cover the possibility of infection caused by uncommon organisms. The approach generalized from management of neutropenic, febrile patient, is often used a as a substitute for appropriate diagnostic evaluation;
- ) Pressure from the patient to be treated with an antimicrobial agent;
- ) Time constrains;
- ) Cost and availability of radiographic studies and diagnostic tests in relation to the ready solution offered by prescribing;
- ) Inadequacy of some physicians’ knowledge of diagnostic procedures and management of infectious diseases;
- ) Malpractice considerations and fear of litigation;
- ) “Spiraling empiricism” refers to concerns about increasing prevalence of antimicrobial resistance and the perceived need to prescribe ever more broad spectrum antimicrobials to “cover” these pathogens; and
- ) Easy solutions provided by the manufacturers.
Some clinicians believe that ASPs impose unnecessary or even deleterious constrains on the practice of medicine.24,25 Their skepticism arise from the perception that there is a lack of documented efficacy of ASPs across varied health care settings, a paucity of direct evidence demonstrating an improvement in clinical outcomes, limited time or incentive to pursue such efforts and, a weak causal link between the emergence of resistance and antibiotic use patterns.
Stewardship strategies are as follows:
- ) Antibiotic order forms;
- ) Antibiotic rotation;
- ) Antimicrobial formulary restriction;
- ) Automatic stop orders;
- ) Clinical practice guidelines;
- ) Computer –assisted management programmes;
- ) Costing of items in clinical microbiology laboratory;
- ) Direct interaction;
- ) Educational programmes;
- ) Formal seminars;
- ) Multidisciplinary approaches;
- ) Newsletters;
- ) Performance evaluation;
- ) Prior approval programmes;
- ) Purchase plans;
- ) Simple chart entry;
- ) Telephone approval; and
- ) Therapeutic substitution and streamlining programs.
This analytical cross-sectional study was carried out in the Critical Care Center of Combined Military Hospital, Dhaka Cantonment, Bangladesh from April 2016 to July 2016. Admitted patients in Critical Care Centers (CCC) with clinically diagnosed conditions Including fever, diabetes mellitus with or without complications (DM), coma, single or multi-organ organectomy and more were included in the study. Following strict aseptic precautions and standard procedures, midstream clean catch urine and other specimens were collected was done. Approval of appropriate authority was taken for conduction of the study. Data were analysed for patients showing positive culture, in AFIP, Dhaka Cantonment from these, the pattern of isolate and sensitivity pattern were evaluated after employing standard microbiological method of bacterial identification and sensitivity by Kirby-Bauer disc diffusion method. Finally, Microsoft excel data analysis tool were used for analysis for result generation.
Sample collection: Urine and other samples were collected for the bacteriological examination from the critical care set up of CMH Dhaka. Collection of midstream clean catch urine was adopted and other specimen collections were done following strict aseptic precautions. Transportation of specimens was carried out carefully to the laboratory.
Isolation and identification: The collected samples were cultured into blood agar and MacConkey agar media. Appropriate and specific procedure were followed for morphological and biochemical identification of the isolated organisms.
Antimicrobial susceptibility test: Susceptibility pattern were performed using disc diffusion method in Mueller-Hinton agar plate. Cultures were tested against antibiotics in common use in management of patients. The proportion of ineffective antimicrobials was calculated as the sum of the resistant isolates relative to the total number of drug tested. The organisms were more such agents, considered multi drug resistant (MDR) when showing resistance to the effect of three or more.
Out of 1670 specimens, 190 showed positive culture yield. E. coli was the most frequent organisms isolated from the 116 urine specimens.(table I)
Organism |
Total number |
Percent |
E coli |
82 |
70.69 |
Enterococci |
11 |
9.48 |
Pseudomonas |
3 |
2.59 |
Klebsiella |
8 |
6.90 |
Acinetobacter |
6 |
5.17 |
Proteus |
0 |
0 |
Staph aureus |
3 |
2.59 |
Enterobacter |
2 |
1.72 |
Candida |
1 |
0.86 |
Antibiotic sensitivity of the isolates to used doses of the various antibiotics studied in urine specimen isolates, showing 58.41% sensitive to Azithromycin (table-II).
Antibiotic |
Resistant |
Percent |
Antibiotic |
Resistant |
Percent |
Azithromycin |
66 |
58.41 |
Aztreonam |
9 |
90.00 |
Ciprofloxacin |
66 |
58.41 |
Netilmycin |
2 |
20.00 |
Ceftriaxone |
75 |
65.79 |
Gentamicin |
2 |
33.33 |
Ceftazidime |
75 |
72.82 |
Amikacin |
2 |
22.22 |
Nitrofurantoin |
62 |
60.78 |
Meropenem |
9 |
100.00 |
Nalidixic acid |
70 |
69.31 |
Cefepime |
6 |
75.00 |
Cefuroxime |
76 |
73.79 |
Pipercillin+Tazo |
9 |
60.00 |
Livofloxacin |
15 |
15.15 |
Erythromycin |
10 |
76.92 |
Linezolid |
15 |
11.11 |
Carbenicillin |
1 |
100.00 |
Amoxyclav |
80 |
73.40 |
Others |
2 |
50.00 |
Colistin |
0 |
0 |
|
|
|
Vancomycin |
1 |
9.10 |
|
|
|
Penicillin |
8 |
61.54 |
|
|
|
Resistance trends of all the antibiotics used in urinary isolates,indicatedmore antibiotics wereresistant in the isolates than sensitive. Sensitivity pattern of first eight isolates from urine specimens, clearly shownthat about 60% resistant and only about 40% sensitive (figure 1).
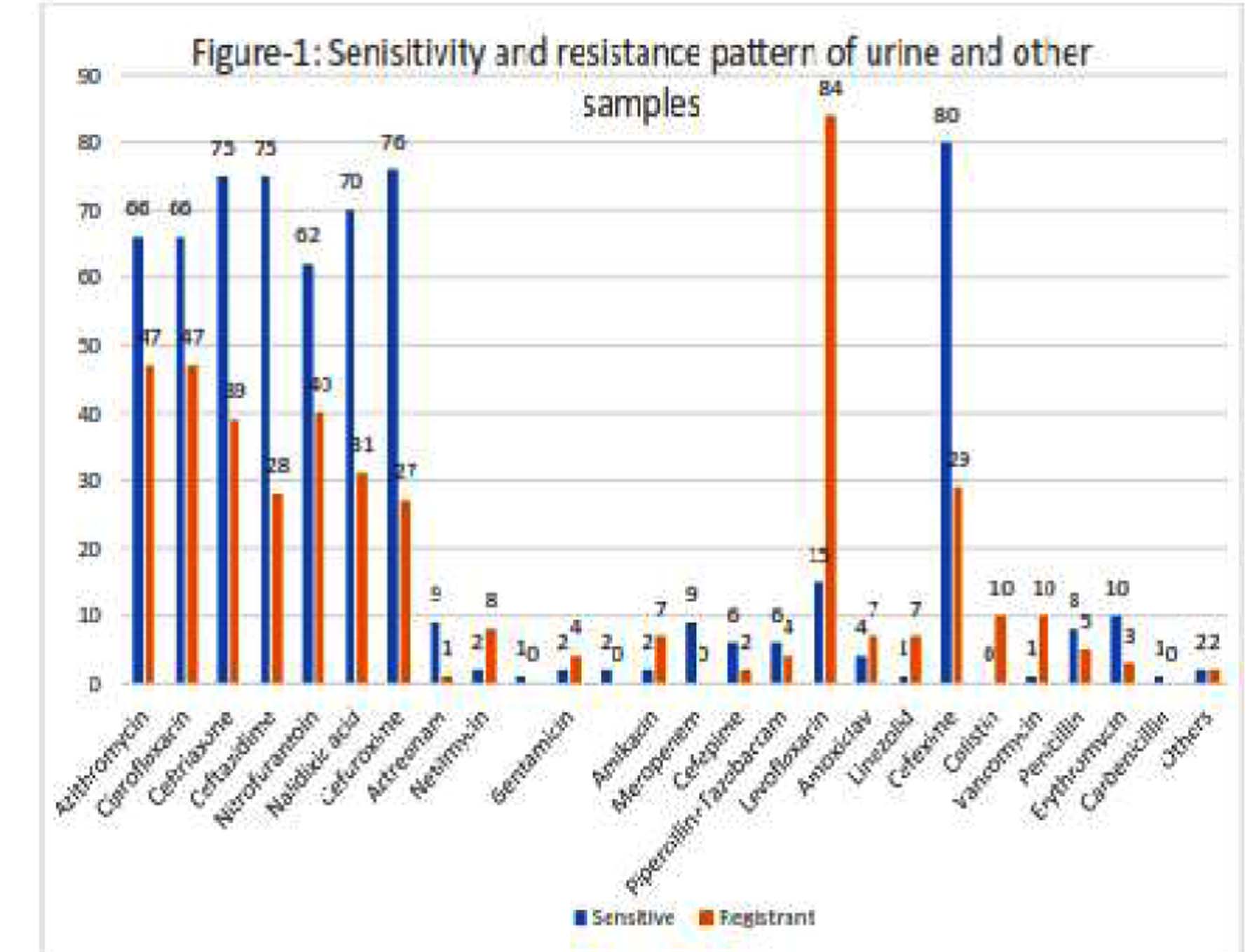
The percentof sensitivity/resistance weredelineated along with percent of disc used in first seven urinary specimens.Isolate number in other specimensshowed highest number of acinobacter(table-III).
Organism |
Total number |
Percent |
E coli |
16 |
21.62 |
Staph auresus |
11 |
14.86 |
Acinetobacter |
18 |
24.32 |
Enterococcus |
6 |
8.11 |
Klebsiella |
7 |
9.46 |
Streptpneu |
6 |
8.11 |
Proteus |
4 |
5.41 |
Pseudomonas |
4 |
5.41 |
Salmonella |
2 |
2.70 |
Sensitivity and resistance pattern of the isolates in other specimensindicated 18 (24.32%) Acinetobacter, the most frequent yield followed by E coli 16 (21.62%) and Staphylococcus aureus 11 (14.86%)(tableIV).
Antibiotic |
Resistant |
(%) |
Antibiotic |
Resistant |
(%) |
Azithromycin |
38 |
52.05 |
Aztreonam |
20 |
100 |
Ciprofloxacin |
28 |
37.84 |
Netilmycin |
11 |
52.38 |
Ceftriaxone |
36 |
49.32 |
Cefepime |
19 |
90.48 |
Ceftazidime |
30 |
61.22 |
Pipercillin +Taz |
19 |
95.00 |
Nitrofurantoin |
1 |
100 |
Livofloxacin |
7 |
30.44 |
Nelidixic acid |
1 |
50 |
Amoxyclav |
46 |
63.89 |
Cefuroxime |
36 |
78.26 |
Linezolid |
1 |
12.50 |
Cefixime |
41 |
56.94 |
Cephalexin |
41 |
75.93 |
Colistin |
2 |
9.52 |
Flu,Clo,Pef |
00 |
0 |
Vancomycin |
0 |
00.00 |
Other |
35 |
72.92 |
Penicillin |
15 |
65.22 |
|
|
|
Erythromycin |
5 |
21.74 |
|
|
|
Gentamicin |
0 |
Nu* |
|
|
|
Meropenem |
0 |
Nu* |
|
|
|
*Not used
Periodical surveillance of the prevalent isolate pattern and their antimicrobial susceptibility are valuable information for determination of appropriate therapy for infections in critically-sick patients.26The study, recorded two Enterobacter spp isolates in urine specimen, one is only Colistin sensitive, another is sensitive to Netilmycin and Amikacin in addition to Colistin. This study did not include any VRE. It is evident from the record that irrespective of the complain(s), patients weregiven more than one antibiotic management in CCC. Isolate yield in specimen of urine with E coli as the most frequent organism 82 (70.69%) followed by Enterococci, and least is Enterobacter only 2 (1.72%). Most sensitive were Colistin (100%), Linezolid 15(11.11%), Netilmycin 2(20.00%), Amikacin 2 (22.22%) andGentamicin 2 (33.33%). Most resistant were Meropenem and Carbenicillin 9, 1 (100.00%) used respectively; then Aztreonam, Erythromycin, Cefepime and Cefuroxime. The sensitivity pattern of the used antibiotics highest activity weredelineated by Flucloxacillin, Cloxacillin, Pefloxacillin, Ofloxacillin and Vancomycin, all appeared sensitive in the study. Colistin and Linezolid come next in efficacy. Most resistant wereNitrofurantion, Cefuroxime, Cephalexin, Cephradin.Prevalence of resistance ratesexpressed in earlier works are fewer than it is now, 25% as a whole in 2013, an indication of gravity of the antibiotic resistance problem. The result indicated that these organisms werein possession of drug resistance acquired due to empiric or prophylactic antibiotics applied prior to obtaining sensitivity pattern of the growth. About 60% of the used antibiotics wereresistant in isolates, and they werenosocomially gained infection in CCC setup. The study didnot include finding out the exact cost in the purchase of antibiotic drug in the CCC set up in CMH, reliable source indicate it to be above 60% of drugs budget. A survey in 47 hospitals in phase 3 Project ICARE (Intensive Care Antimicrobial Resistance Epidemiology) revealed that all hospitals had an antimicrobial formulary and 91% of them used at least one of the following three mechanisms to improve use: stop orders, antibiotic restriction, or clinical practice guidelines. Antibiotic resistant bacterial nosocomial infections are a leading problem in intensive care units (ICU). To study the pattern of microorganism and bacterial resistant to antibiotic in ICU of Bangabandhu Sheikh Mujib Medical University (BSMMU) of Bangladesh a similar study, as the one in question was carried out.27 The causal link between the use of antibiotics for animal growth promotion and augmentation of resistance in human pathogens has been disputed28, but more recent evidence is convincing that transfer of resistance gene occurs through the food human consume.28,29It was reported that, aquatic environments are particularly rich in bacterial population replete with antibiotic resistance genes30. A Vancomycin resistantE coliwasisolated in urine specimen in the study. Reports of VRSA in Japan and the United States showed that common, invasive microbial pathogens may become refractory to any chemotherapeutic agent in future. 31
Analysis of bacterial resistance to antibiotics in south east Asian region revealed that multi drug resistant (MDR) Tuberculosis, extended drug resistant TB (XDR) reported from Bangladesh, India, Indonesia and Thailand. 32
A report recommends total volume of antibiotic prescribing quinolones, cephalosporins, coamoxyclav and other broad spectrum agents as well as 3 days course for trimethoprim, nitrofurantoin and pivmecillinum.33 Poor public health indicators, rising incomes, and the availability of inexpensive antibiotics over the counter without a prescription are converging to create the ideal conditions for a large-scale selection and dissemination of resistance genes in India. India is not alone in this battle, and the experiences of other countries in dealing with antimicrobial resistance are described in the most recent State of the World’s Antibiotics Report 34.
It may be concluded that the appropriate surveillance, a hospital laboratory may efficiently and rapidly detect the emergence of new resistance, or the presence of a new microbial strain, within a specific unit or patients. Work on the clinical presentation, with the trends of antimicrobials used in the CCC setup in tertiary care hospital would be of complemented value tothe study for further steps towards implementation of antibiotic stewardship programme.
The authors gratefully acknowledge the technical support of the Bangladesh Medical Research Council. The authors are also thankful to colleagues from AFIM and CMH, Dhaka for their cooperation and support
Conflict of Interest: There is nopotential conflict of interest of any of the authors in this study.
References
- T A Russo, J R Jonson. Diseases caused by Gram Negative Bacteria. In: D L Longo, D L Casper, J L Jameson, A S Fauci, S L Hauser, J Loscalzo, editors. Harrisons Principles of Internal Medicine Vol 1, 18thed. New York, Chicago: MacGrow Hill; 2012. P. 1247
- D L Longo, D L Casper, J L Jameson, A S Fauci, S L Hauser, J Loscalzo, editors. Harrisons Principles of Internal Medicine, 18thed Vol 1. New York, Chicago: MacGrow Hill; 2012. P. 1246-57.
- RodriguezBaño, LolaGarcía, EncarnaciónRamírez et al. Long-term Control of Hospital-wide Endemic Multidrug-Resistant (MDR) Acinetobacter baumannii through a Comprehensive “Bundle” Approach. https://www.researchgate.net/publication/24441814.
- R A Polk, N O Fishman. Antimicrobial Stewardship. In: G L Mendell, J E Bennett, R Dolin. Mendell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 7thed, Vol 1. Philadelphia: ChurchchillLivingstone,Elsevier; 2010. P 677.
- Jawetz E. Antimicrobial chemotherapy. Annu Rev Microbiol : 1956; 10: 85.
- Cosgrove S, Carmelli Y. The impact of antimicrobial resistance on health and economic outcomes. Clin Infect Dis 2003:36; 1433-1437.
- Muellering RC, Graybill JR, McGowan JE, et al. Antimicrobial Resistance Prevention Initiative-An update: Proceeding of an expert panel on resistance. Am J Med. 2007; 120:S4-S25.
- Hecker MT, Aron DC, Patel NP, et al. Unnecessary use of antimicrobials in hospitalized patients. Arch Intern Med. 2003; 163:972-978.
- Timothy HD, Robert CO, John EM, Dale NG, Robert AW, John PB, W CH, David LP, Neil OF,
- VogtlanderNPJ, van KasterenMEE, Natsch S et al. Improving the process of antibiotic therapy in daily practice: Interventions to optimize timing, dosage adjustment to renal function, and switch therapy. Arch Intern Med. 2004; 164:1206-1212.
- Hidron AI, Edwards JR, Patel J et al. The National Healthcare Safety Network Team and Participating National Healthcare Safety Network Facilities. Anti Microbial –resistant pathogens associated with healthcare –associated infection: Annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention. 2006-2007. Infect Control Hosp Epidemiol. 2008; 29:996-1011.
- Spellberg B, Guidos R, Gilbert D, et al.The epidemic of antibiotic – resistant infections: A call to action for the medical community from the Infectious Diseases Society of America. Clin Infect Dis. 2008;46:155-164.
- Talbot GH, Bradley J, Edwards JE et al. Badbugs need drugs: An update on the development pipeline from the antimicrobial availability task force of theInfectious Diseases Society of America.ClinInfectDis. 2006; 42:657-668.
- McGowan JE Jr, Gerding DN. Does antibiotic restriction prevent resistance? New Horiz. 1996; 4:370-376.
- Sunenshine RH, Liedtke LA, Jernigan DR et al. Role of infectious diseases consultants in management of antimicrobial use in hospitals.Clin Infect Dis.2004;38:934-938.
- Struelens MJ. Multidisciplinary antimicrobial management teams: The way forward to control antimicrobial resistance in hospital. CurrOpin Infect Dis 2003;16:305-307.
- John JF, Fishman NO. Programmatic role of the infectious diseases physician in controlling antimicrobial costs in the hospital. ClinInfect Dis 1997;24:471.
- Dellit TH, Owens RC, McGowan JE, el al.Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America :Guidelines for developing an institutional program to enhance antimicrobial stewardship.Clin Infect Dis 2007; 44:159-177.
- Avorn J, Solomon DH. Cultural and Economic factors that (mis) shape antibiotic use; The (non) pharmacologic basis of therapeutics. Ann Intern Med 2000; 133:128-135.
- Timothy HD, Robert CO, John EM, Dale NG, Robert AW, John PB, W CH, David LP, Neil OF, Christopher FC Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America Guidelines for Developing an Institutional Program to Enhance Antimicrobial Stewardship available fromhttp://cid.oxfordjournals.org/content/44/2/159.full
- 12/30/2015 IDSA Responds to The Joint Commission's Proposed Standards for Antimicrobial Stewardship for Various Types of Healthcare Facilities available from https://www.idsociety.org/Stewardship_Policy/.
- Owens RC Jr Antimicrobial stewardship: concepts and strategies in the 21st century.Diagn Microbiol Infect Dis. 2008; 61:110-28
- Kim JH, Gallisha. Observations on spiraling empiricism: Its causes, allure, and perils with particular reference to antibiotic therapy. Am J Med. 1989;87:201-206.
- Rybak MJ. Pharmacodynamics: Relation to antimicrobial resistance. Am J Med. 2006;119,S37-S44
- McGowan JE Jr. Minimizing antimicrobial resistance: The keyrole of the infectious diseases physician. Clin Infect Dis. 2004;38:939-942.
- Lawton RM, Fridkin SK, Gaynes RP, et al. Practices to improve antimicrobial use at 47 US hospitals; The Status of the 1997 SHEA/IDSA position paperrecommendations. Society for Healthcare Epidemiology of America/Infectious Diseases Society of America. Infect Control Hosp Epidemiol. 2000; 21:256-259
- Patterson D, Rice L. Emperical antibiotic choice for the seriously ill patient: Are minimization of selection of resistant organisms are maximization of individual outcome mutually exclusive? Clin Infect Dis 2003; 36:1006-1012.
- Mondol MK, Roy BR, Yeasmin S, Haque F, Huda AQK, Banik D. Prevalence of microorganism and emergence of bacterial resistance in ICU of Bangabondhu Sheikh Mujib Medical University.Journal of Bangladesh Society of Anaesthetists. 2013; 26: 20-26
- Cattoir V, Poirel L, Aubert C, et al. Unexpected occurrence of plasmid mediated quinolone resistance determinants in environmental Aeromonas spp. Emerg Infect Dis. 2008; 14:231-237.
- Barlam TF DiVall M. Antibiotic-stewardship pactices at top academic throughout the United Sates and at hospitals throughout Massachusetts. Infect Control Hosp Epidemiol. 2006;27:695-703.
- Rice LB. The Maxwell Finland Lecture; For the duration rational antibiotic administration in an era of antimicrobial resistance and Clostridium difficile. Clin Infect Dis. 2008;46:491-496.
- Levy SB. Antibiotic resistance: Consequences of inaction. Clin Infect Dis. 2001; 3: S124-S129.
- Review of regional workshop on antimicrobial resistance Bangkok Thailand. 6-10 Aug 2012
- Antimicrobial stewardship: prescribing published: 15 June 2015.NICE(National Institute of Health care and excellence), UK.
- Antibiotic resistance and Use in India. CDDEP. The State of the World's Antibiotics, 2015. Washington DC: Center for Disease Dynamics, Economics & Policy2015.